
Most of the time, ECMO programs are focused on warming patients, not cooling them. The extracorporeal circuit pulls a large volume of blood through tubing exposed to ambient air, and without active warming it draws heat out of the patient as it runs. Plus, the patients themselves also tend to arrive cold, from shock, prolonged resuscitation, massive transfusion, or intraoperative cooling.
But climate change is driving longer and more intense heat waves, and heat-related ICU admissions are rising year over year. As a result, we may start to see more patients placed on ECMO for heat stroke, an application of the therapy that has thus far been quite rare.
Heat Stroke 101
Heat stroke is a life-threatening emergency defined by a core body temperature above 40° C (104° F) along with central nervous system dysfunction. Despite the name, the ‘stroke’ in heat stroke isn’t a reference to a cerebrovascular event. It uses the word’s original meaning of ‘a sudden blow,’ describing the abruptness of the presentation: a patient upright one moment and incapacitated the next. It comes in two forms:
- Classical heat stroke: develops slowly in vulnerable populations during environmental heat exposure, often in elderly patients during heat waves.
- Exertional heat stroke: develops rapidly in younger, otherwise healthy individuals during physical exertion in hot conditions.
Both can progress to multi-organ failure if not recognized and treated quickly. Common patterns of organ involvement include:
- Brain dysfunction: confusion, agitation, delirium, seizures, coma, or lasting neurologic injury.
- Muscle breakdown: heat and exertion can trigger rhabdomyolysis, where muscle tissue breaks down and releases proteins/electrolytes into the blood.
- Kidney injury: dehydration, shock, and rhabdo-related myoglobin can cause acute kidney injury, sometimes requiring dialysis.
- Liver and clotting dysfunction: severe heat stroke can cause hepatic injury and coagulopathy/DIC, where clotting becomes abnormal and dangerous.
- Lung/cardiovascular collapse: severe cases can involve ARDS/respiratory failure, shock, arrhythmias, and multi-organ failure.
Cool First, Then Consider ECMO
On paper, ECMO for heat stroke seems like a no-brainer. The circuit’s heat exchanger makes precise temperature control easy in either direction, exactly what a refractory hyperthermia case calls for (albeit more invasive than other cooling options). And for the lung and cardiovascular collapse the most severe patients can develop, ECMO is already the salvage tool clinicians reach for in other settings. So why is it so rare to actually see these patients on the circuit?
A couple of reasons. First, heat stroke doesn’t present the same way for everyone. One patient is in status epilepticus, another is bleeding from DIC, another is in refractory shock. The dominant clinical picture varies enough that ECMO ends up being a decision made case by case rather than by protocol. Second, the cooling data. If you cool a patient quickly and effectively, most of the downstream organ damage can be prevented or limited.
This leaves ECMO with a narrower role. It is not first-line care, and most heat stroke patients should not need it. The patients who do are typically those who arrived late, were cooled inadequately, or presented already in refractory shock or arrest.
What Defines Adequate Cooling?
Adequate cooling is defined as lowering the core temperature by 0.15 to 0.35° C per minute. Current guidance points to cold water immersion as the first-line treatment whenever the patient can tolerate it, with the patient submerged up to the neck in ice water for rapid whole-body cooling. When a proper tub isn’t available, tarp-assisted cooling offers the same physiology in the field, with the patient laid on a tarp held up at the corners and filled with ice water around them.
Evaporative cooling, where the patient is sprayed with water and exposed to fans, is the most practical alternative for elderly classical heat stroke patients who can’t tolerate immersion, though it cools more slowly. Ice pack application and cold saline infusion are typically used as adjuncts rather than primary treatment because they don’t reliably cool the patient fast enough.
Endovascular cooling catheters and surface cooling pads are also part of the picture, though they tend to come into play after the patient reaches the ED or ICU rather than during the initial cooling phase. Because rapid temperature reduction is the priority in the first minutes after presentation, the early cooling work usually happens in the field
ECMO only enters the picture when the patient has progressed beyond what these tools can fix, or when other organ failures demand extracorporeal support regardless of temperature.
What the ECMO Literature Looks Like Today
The published evidence for ECMO in heat stroke is sparse. There is no randomized controlled trial, no ELSO consensus statement, and no dedicated systematic review of outcomes. What does exist is a small collection of single-patient case reports, scattered across journals and across the world.
As climate-driven heat stroke increases, this body of literature is starting to grow. But even with its current limits, the published cases are worth examining for what they reveal about who has been cannulated, in what configurations, and how those decisions played out.
Case 1. An Elderly Japanese Man in a Hot Bath
According to a 2021 case report, a 68-year-old man was found unconscious in a hot bathtub on a winter day in Japan. He arrived with a core temperature of 40.5°C, a Glasgow Coma Scale of 4, a systolic pressure of 65 mmHg, and visibly flushed skin. He was cooled with body surface ice packs, intragastric cold water, and cold IV fluids, dropping his core temperature to 37°C within an hour.
However, shortly after, his circulation collapsed, with systolic pressure dropping to 30 mmHg despite escalating vasopressors, likely driven by the distributive shock heat stroke’s inflammatory cascade can produce even after cooling. He was placed on VA-ECMO six hours after arrival, weaned by day 3, and discharged after 116 days in the hospital.
Case 2. An Outdoor Worker in Status Epilepticus
Another case study described a 64-year-old man with exertional heat stroke after outdoor occupational heat exposure, who arrived with status epilepticus and a core temperature of 40.9°C. Conventional cooling failed to bring his temperature down, and his ongoing seizures and hyperthermia left him in acute respiratory failure despite intubation.
VV-ECMO was placed to address both problems at once, taking over gas exchange while the heat exchanger delivered rapid and precise cooling. He reached target temperature within half an hour, his seizures resolved as he cooled, and he was discharged on day 8 with no deficits.
Case 3. A Young Worker with Cascading Organ Failure
Li and colleagues described a 34-year-old man who collapsed after working in extreme heat, arriving with multi-organ failure including renal injury, hepatic injury, and DIC. Standard surface cooling was slow, so the team initiated CRRT with cold replacement fluid, which dropped his rectal temperature into a safer range within three hours.
Yet, by day 2, the inflammatory cascade and capillary leak that heat stroke can trigger had progressed into heat-induced ARDS, with hypoxemia outpacing what mechanical ventilation could correct, and VV-ECMO was added for gas exchange. Both ECMO and CRRT were weaned on day 9, and he was discharged from the ICU on day 15.
A Loose Decision Tree for the Bedside
These three cases don’t give us a protocol, but they suggest a sequence of questions to work through when a heat stroke patient is in front of you.
The decision tree below maps out the logic visually, but in words, here’s how the cascade goes:
First: is cooling working? If standard methods are bringing the temperature down adequately, the path forward is supportive care and watchful management of the complications that may still develop (some of which may still call for ECMO).
If cooling isn’t working with first-line methods, the next question is whether the patient already has an indication for ECMO. If there’s heart or lung involvement that would call for cannulation anyway, ECMO can solve both problems at once. If not, escalating to endovascular cooling or surface pads is usually the more reasonable next step, since cannulation for cooling alone is generally too invasive of an intervention to justify.
The choice between VV and VA essentially comes down to whether the heart is compromised. If the patient is in refractory shock or arrest, VA gives circulatory support and an oxygenator. If cardiac function is preserved and the dominant problem is cooling, ventilation, or both, VV is the more logical configuration.
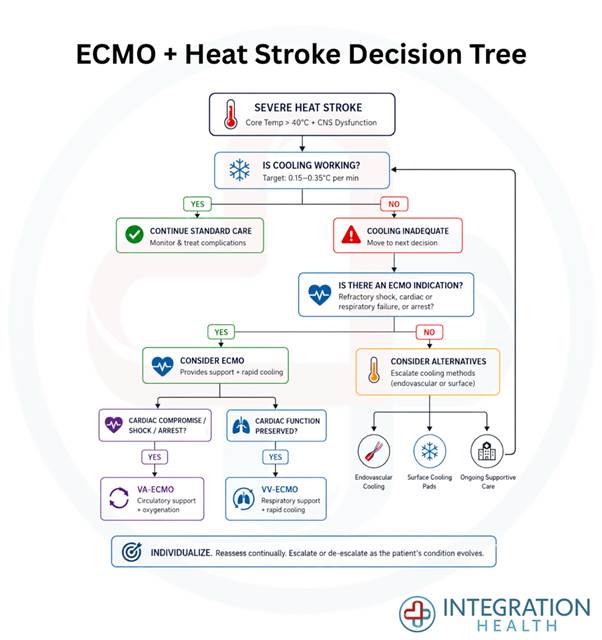
The decision tree above is not a rigid algorithm, but rather a way to think through these cases; the evidence base is too thin, the patient phenotypes too varied, and the published cases too few to support anything firmer.
But with heat waves intensifying and heat-related ICU admissions rising every summer, more clinicians are likely to find themselves having this conversation at the bedside in the coming years, and the small body of literature these cases belong to will start to grow alongside the patient population.


